Heritability of Hip Dysplasia in Dogs
Hip dysplasia is one of the clearest examples of a trait that is both genuinely heritable and still not individually predictable, and the combination is important enough to pause on before either half of the sentence slips away. The literature strongly supports that genetic differences matter, that selection works, and that phenotype-based screening has improved populations over time. It also supports that hips are polygenic, developmentally modulated, and never reducible to one simple genetic answer. Holding both sides of that picture at once is the whole challenge of communicating about hip dysplasia honestly, and breeders who collapse it into either pure genetics or pure environment end up misleading families in opposite directions. Documented
What It Means
The disease as a developmental orthopedic problem
Hip dysplasia is a developmental orthopedic disease rooted in joint laxity, altered loading patterns, and the later progression to osteoarthritis as the joint surfaces wear unevenly over years of use. The primary anatomical feature is a hip joint that fits together less tightly than it should, with a ball and socket whose congruence is reduced during the critical period of skeletal development. That laxity means the joint experiences forces it is not shaped to handle, and the body's response to abnormal loading over time is cartilage damage, bone remodeling, and eventually the arthritic changes that cause the clinical pain and reduced mobility families recognize as the disease.
That developmental framing matters for how the genetics should be interpreted. Hip dysplasia is not a structural birth defect that is fully present at the moment a puppy is born. It is a condition that unfolds during the months when the skeleton is growing, the soft tissues are maturing, and the joint is taking on its adult shape under the combined influence of genetic predisposition and mechanical load. Two puppies can start life with similar hip conformation at eight weeks and end life in very different orthopedic places, and the difference is the combined consequence of their underlying genetic liability and the developmental conditions they experienced along the way.
The polygenic architecture
From a genetics perspective, the important point is that the trait is polygenic. There is no single hip-dysplasia gene whose presence or absence settles the question. Instead, many loci across the genome each contribute small amounts of liability, and the total genetic contribution to any individual dog's hip phenotype is the sum of contributions from many places in the genome rather than the reading of one diagnostic marker.
That polygenic architecture is why simple DNA tests for hip dysplasia have struggled to deliver the precision families often want. A single-locus test can work cleanly for a condition with one causal mutation, but hip dysplasia is not that kind of condition. Even polygenic risk score approaches, which try to aggregate the effects of many small-contribution variants into a single number, have faced real difficulties in dogs because the effect sizes of individual loci are small, the populations being studied are often small relative to what is needed for robust statistical estimation, and the phenotype itself is noisy enough that the signal-to-noise ratio in genomic prediction is not yet where it needs to be for confident individual-dog forecasts. Observed-JB
That means two things can be true at once. The trait is heritable in the formal quantitative sense. And the phenotype is still developmentally modulated, polygenic, and not cleanly readable from a DNA swab with current technology. These are not contradictions; they are complementary features of how complex traits work in any mammalian species.
Interpreting the heritability number
Published heritability estimates for hip dysplasia vary by breed, population, scoring method, and the specific phenotype being measured. Many studies place hip-dysplasia-related traits in a low-to-moderate heritability range, often around 0.2 to 0.4, though some estimates run higher or lower depending on what exactly is being measured. Estimated Whether the phenotype is joint laxity measured via PennHIP distraction index, a radiographic subjective score like the OFA hip grade, a direct measurement of femoral-head congruence, or an aggregate grade combining multiple features, the resulting heritability estimate can differ noticeably because the different phenotypes are not the same underlying trait even though they correlate with one another.
A heritability value in the 0.2 to 0.4 range means that in the studied population, somewhere between about a fifth and two fifths of the observed variation between dogs in that hip phenotype was attributable to additive genetic differences. Estimated That is enough to support meaningful response to selection, but it is also not so high that the other sixty to eighty percent of variation can be ignored. The environmental and developmental contribution to hip phenotype is substantial even in breeds where the genetic contribution is well established, and that combined picture is what responsible breeding has to work with.
This is why the question "Is hip dysplasia genetic or environmental?" is badly formed in a way that produces confused breeding conversations. The answer is yes to both, and insisting on a binary answer hides the structure of how the disease actually develops. The genes create liability. Growth rate, body condition, developmental load, nutrition, and exercise history can influence how that liability expresses in the individual dog. Families who understand this can make better decisions about both which breeder to choose and how to manage the puppy they bring home.
Selection response as the strongest proof
The strongest practical proof that hip dysplasia heritability is real is not the coefficient itself, which is often treated with more precision than the underlying measurements can support. Observed-JB It is the documented response to selection. In multiple dog populations across multiple breeds, sustained phenotype-based breeding pressure (meaning that breeders have consistently selected for better hip scores in breeding candidates over many generations) has produced measurable reductions in dysplasia prevalence. That response is exactly what quantitative genetics predicts for a trait with real additive genetic variance, and the fact that it has happened in the real world, not just in theoretical models, is what makes hip heritability more than a statistical curiosity.
The response-to-selection evidence is also what rescues the concept of screening from the skepticism it sometimes attracts. A critic might argue that heritability estimates are noisy, that screening methods are subjective, and that environmental factors confound everything. All three concerns have merit. But none of them can explain why breed populations actually saw dysplasia rates decline under consistent screening pressure. If the genetic component were not real, selection would not have worked, and the improvements would not have materialized. They did, across many breeds and many decades, and that outcome is the evidence most worth anchoring on.
Why phenotypic screening remains central
This is also why phenotypic screening remains central to responsible hip management rather than being superseded by DNA-based alternatives. Hips are not one of the traits where DNA testing presently gives the cleanest practical answer. Direct radiographic evaluation of the joints, whether through the OFA grading system, PennHIP distraction testing, or other recognized protocols, still tells breeders more about what they need to know than any currently available genetic prediction.
The reason is partly the polygenic architecture described above and partly the measurement problem. Phenotypic screening measures the thing being selected for directly (the state of the actual joint), while genomic prediction measures a proxy (the dog's DNA profile) and then infers the phenotype from the proxy. When the proxy-to-phenotype map is well understood, as it is for simple Mendelian conditions, genomic prediction can be powerful. When the map is complex and noisy, as it is for hip dysplasia, measuring the phenotype directly remains the more reliable option.
That may change in the future as canine genomic databases grow, as more dogs are phenotyped and genotyped together, and as polygenic prediction methods improve. Documented Responsible breeders should stay open to incorporating new tools as they become validated. But the current state of the science is that phenotypic screening is the main practical tool, and families should treat any breeder who claims to rely on DNA testing alone for hip management as likely overstating what the science currently supports.
The gene-environment interplay in practice
The environmental modulation of hip expression is not hypothetical. Growth rate matters, because puppies grown too fast on excessive calories are thought to load developing joints in ways that can worsen expression of underlying liability. Body condition matters, because excess weight on a growing skeleton adds mechanical stress that the joint was not shaped to handle. Exercise patterns matter, because repeated high-impact activity on immature joints is different from normal developmental movement, and some evidence suggests that both too much and too little movement during critical growth periods can influence outcomes in ways the breeding community is still working to quantify precisely.
None of this absolves breeders of responsibility for selecting parents with good hip phenotypes. It means that a responsible program treats hip health as a combined project of genetic selection and developmental husbandry rather than assuming that one layer alone is sufficient. A dog with excellent genetic liability can still develop dysplasia under poor growth management. A dog with moderate genetic liability can still end up with functional hips under careful growth management. Both facts are consistent with the heritability literature, and both should inform how breeders talk to families about what they can and cannot guarantee.
Why It Matters for Your Dog
Families usually want a clear answer about whether a litter is low-risk. Observed-JB The honest breeder answer is more nuanced than families sometimes expect, and the nuance is not evasion. It reflects how the disease actually works.
Low-risk is built from layers rather than from any single test result. The parental phenotype, evaluated through recognized screening methods and confirmed on multiple dogs in the line, is one layer. The long-term line history, meaning what happens to the puppies produced by the breeding program as they reach adulthood and old age, is another layer, and often a more informative one because it captures what the phenotypic scores actually predict in practice. Diversity management matters because narrow lines can concentrate polygenic liability in ways that single tests do not always reveal. And puppy growth and body-condition management after the family takes the dog home is the final layer, which shifts some of the responsibility onto the family rather than leaving everything at the breeder's door.
That is why the best breeders do not talk about hips as though one test result ended the conversation. They talk about hips as a selection project running across generations, combined with an ongoing husbandry project that continues into the family's hands. That framing is harder to compress into a marketing slogan than "all our parents are OFA Good" but it is closer to what the biology actually supports, and families who understand it are better equipped to partner with the breeder over the dog's lifetime.
For JB, that matters because orthopedic soundness is part of the biological base that lets the raising philosophy work. A dog carrying chronic joint pain is less able to remain calm, stable, and socially useful inside the raising environment that the program depends on, and the Five Pillars are much harder to apply to a dog whose body is limiting what its nervous system can do. Health and temperament are not separate silos in real life, and the program's emphasis on hip screening is not an unrelated health add-on but part of the same integrated commitment to producing dogs that can actually live the life the philosophy describes.
What This Cannot Predict
Hip heritability cannot tell you whether one specific puppy will become clinically dysplastic, because the individual outcome is not the same as the population-level variance structure that heritability actually describes.
It cannot make a good parental phenotype into a guarantee, because the genetic contribution is polygenic and the environmental contribution is substantial, and even the best parents can produce individual puppies that end up at the unfavorable tail of the distribution.
It cannot make environmental management irrelevant, because growth, body condition, and developmental load continue to influence expression throughout the puppy's early life and into young adulthood.
And it cannot justify presenting any current DNA-based hip prediction as if it were a diagnosis, because the polygenic architecture and the measurement challenges mean that direct phenotypic evaluation still carries more practical weight than any simplified genetic risk score the current market offers.
The population-level rule has to be stated plainly here: hip dysplasia heritability describes how much of the between-dog variation in a population is attributable to genetic differences under the conditions of that particular study. Documented It does not predict the outcome for one puppy with certainty, and any breeder presenting it that way is overstating what the science actually shows.
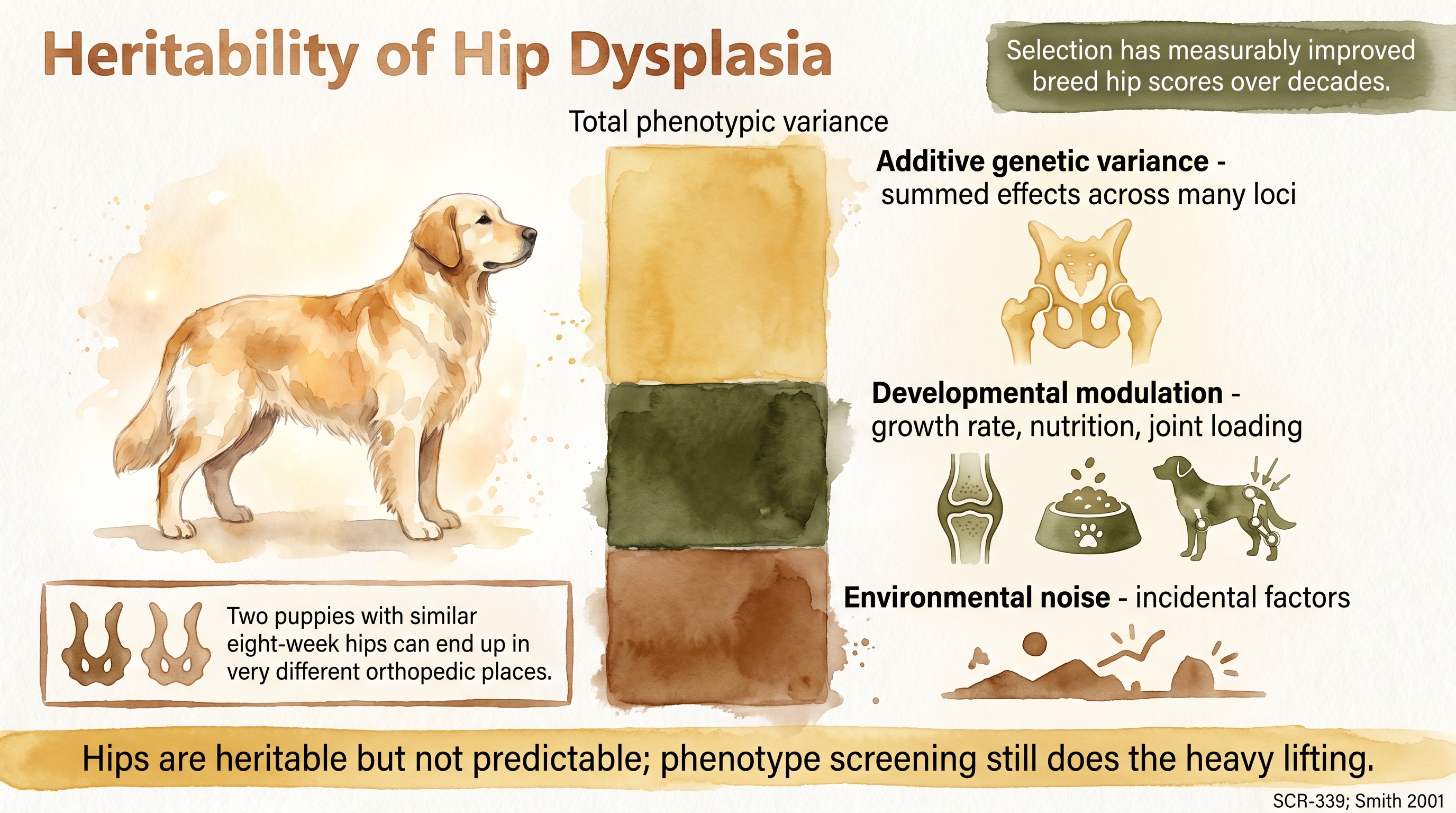
Hips are heritable but not predictable; phenotype screening still does the heavy lifting.
Key Takeaways
- Hip dysplasia is a heritable polygenic trait, not a simple one-gene disease.
- Published heritability estimates support real genetic selection, but they do not make individual outcomes predictable with certainty.
- The best proof that hips are heritable is the documented reduction in dysplasia prevalence under sustained breeding selection.
- Phenotype still matters more than any oversimplified DNA claim because hips are influenced by both genes and development.
- Responsible hip management combines parental screening, line history, diversity, and post-placement growth husbandry across the dog's development.
The Evidence
This entry uses observed claim-level tags beyond the dedicated EvidenceBlocks below. These tags mark JB program observation or practice-derived claims that need dedicated EvidenceBlock coverage in a later content pass.
This entry uses estimated claim-level tags beyond the dedicated EvidenceBlocks below. These tags mark approximate ranges or timing claims that should remain bounded by the cited sources.
- Canine orthopedic and quantitative-genetics literaturedogs
Hip-dysplasia-related phenotypes show low-to-moderate heritability in many studied dog populations, commonly in a range that supports measurable response to selection. - Selection-response studies in dogsdogs
Long-term phenotype-based selection has reduced hip dysplasia prevalence in populations with sustained orthopedic screening and breeding pressure. - Hip screening source synthesisdogs
Radiographic phenotype remains the main practical breeding tool because hip dysplasia is polygenic and developmentally modulated rather than a simple one-locus disorder.
- Canine developmental orthopedic literaturedogs
Growth rate, body weight, and developmental environment can influence the expression of hip dysplasia in genetically predisposed dogs without negating the heritable component.
No randomized controlled trial has directly compared long-term hip outcomes in puppies from screened parents raised under different growth-management protocols across all relevant dietary and exercise conditions.
SCR References
Sources
- Smith G.K., Biery D.N., & Gregor T.P. (1990). New concepts of coxofemoral joint stability and the development of a clinical stress-radiographic method for quantitating hip joint laxity in the dog. Journal of the American Veterinary Medical Association, 196(1), 59-70.
- Smith G.K., Mayhew P.D., Kapatkin A.S., McKelvie P.J., Shofer F.S., & Gregor T.P. (2001). Evaluation of risk factors for degenerative joint disease associated with hip dysplasia in German Shepherd Dogs, Golden Retrievers, Labrador Retrievers, and Rottweilers. Journal of the American Veterinary Medical Association, 219(12), 1719-1724. doi:10.2460/javma.2001.219.1719
- Smith G.K., Paster E.R., Powers M.Y., Lawler D.F., Biery D.N., Shofer F.S., et al. (2006). Lifelong diet restriction and radiographic evidence of osteoarthritis of the hip joint in dogs. Journal of the American Veterinary Medical Association, 229(5), 690-693. doi:10.2460/javma.229.5.690
- Heyman S.J., Smith G.K., & Cofone M.A. (1993). Biomechanical study of the effect of coxofemoral positioning on passive hip joint laxity in dogs. American Journal of Veterinary Research, 54(2), 210-215.
- Leighton E.A. (1997). Genetics of canine hip dysplasia. Journal of the American Veterinary Medical Association, 210(10), 1474-1479.
- Swenson L., Audell L., & Hedhammar Å. (1997). Prevalence and inheritance of and selection for hip dysplasia in seven breeds of dogs in Sweden and benefit:cost analysis of a screening and control program. Journal of the American Veterinary Medical Association, 210(2), 207-214.
- Krontveit R.I., Nødtvedt A., Sævik B.K., Ropstad E., & Trangerud C. (2012). Housing- and exercise-related risk factors associated with the development of hip dysplasia as determined by radiographic evaluation in a prospective cohort of Newfoundlands, Labrador Retrievers, Leonbergers, and Irish Wolfhounds in Norway. American Journal of Veterinary Research, 73(6), 838-846. doi:10.2460/ajvr.73.6.838