What Canine Genetic Tests Actually Predict
The phrase "genetic testing" sounds singular, but dog DNA testing actually covers several very different kinds of tools. Some answer narrow, high-confidence questions. Others provide association-based probability estimates that are directionally useful but cannot guarantee individual outcomes. Others describe a dog's place in the population rather than predicting disease at all. If families do not keep those categories separate in their minds, genetic testing starts sounding much more certain and more comprehensive than it really is, and breeder marketing language often makes the confusion worse by describing all these tools under the single umbrella of "DNA tested" without distinguishing what is actually being measured or how confident the results are. This page exists to give families and breeders a mental map for reading any genetic testing claim they encounter. Documented
What It Means
Four categories, four levels of confidence
The clearest way to understand canine genetic testing is to separate the field into four broad categories based on what the test is actually measuring and how confidently the result can be interpreted. These categories are not always labeled clearly on commercial panels, and some panels mix tests from all four categories onto a single report without distinguishing them, which is one of the ways consumers get confused. But the categories really are different at the biological level, and treating them as equivalent is a category error that leads to poor decisions.
1. Causal-variant Mendelian tests
These are the strongest tests in the field. They identify the actual disease-causing variant, or a mutation treated as causative with strong validation evidence, in a Mendelian disorder where the inheritance pattern is well established and the biological mechanism is understood. Documented The test is directly interrogating the mutation that causes the disease, not a statistical proxy for it, and the interpretation follows classical Mendelian logic.
When a test is in this category, breeder interpretation can be near-binary: clear, carrier, or affected or at-risk depending on the inheritance pattern. For autosomal recessive diseases, those three categories map directly onto distinct mating strategies. For autosomal dominant diseases, the category structure is different but equally clear. For X-linked diseases, sex-specific interpretation applies but the underlying logic remains crisp.
This is the part of canine DNA testing where confidence can be high, provided the mutation and the breed context are both well established. Several Golden Retriever retinal disease tests fall into this category, as do a number of well-validated tests for conditions like exercise-induced collapse, neuronal ceroid lipofuscinosis, and some forms of ichthyosis. When a breeder says a dog is clear for one of these, the statement is doing real work and deserves real confidence. Families should feel comfortable treating those results as close to definitive for the specific locus tested.
The caveat is that even the strongest Mendelian test only covers the specific mutation it was designed to detect. A dog clear for PRA1 is not necessarily clear for PRA2 or for any of the other retinal disease variants that exist in the breed's gene pool. Testing thoroughness requires running all the relevant tests, not just one or two with the highest profile.
2. Linkage-based marker tests
These tests identify a marker associated with a disease locus rather than always identifying the final causal mutation itself. Documented The marker was chosen because it was statistically associated with disease in the study population, and it sits close enough to the actual causal variant to track with it most of the time in that population.
That can still be useful, but the interpretation is more conditional than a causal-variant test. Marker performance depends on the linkage structure in the population where the test was validated, and the long LD blocks in dog breeds mean the marker may be a considerable distance from the actual causal variant. Within the original breed, the marker and the cause almost always travel together, so the test works well as a diagnostic. Move to a different breed or a different haplotype background, and the signal may weaken or disappear because the historical recombination events in the new population have separated the marker from the cause.
This is why the phrases "associated with" and "causes" must not be treated as synonyms, and why breed-specific validation matters so much for marker-based tests. A marker that is reliable in Labrador Retrievers may be useless in Golden Retrievers, and vice versa, even if the test panel advertises it for both breeds. Families should ask whether a marker-based test has been specifically validated in the breed of the dog being tested, and breeders should be cautious about overselling confidence in markers that have only been validated in a single population.
3. Polygenic risk scores
These are the most easily misunderstood tests. For complex traits such as orthopedic liability, cancer susceptibility, or some behavior-related domains, the test may aggregate many loci into a single combined risk estimate. Documented The score summarizes the cumulative contribution of many small genetic effects into a population-level probability statement about the dog being tested.
That estimate is not a diagnosis. It is a probability, and the probability applies to the population the test was developed in rather than to any individual dog with certainty. A high score means the dog is in a higher-risk tier than average; a low score means the dog is in a lower-risk tier than average; neither score guarantees or rules out disease expression. The individual dog is still going to develop or not develop the trait based on its own biology, environment, and life history, and the score is only a starting probability estimate rather than a forecast.
It is not a guarantee, and it does not replace direct phenotype-based evaluation where phenotype is still the gold-standard measure. For hip dysplasia, for example, orthopedic imaging of the actual joints of the actual dog remains more informative than any polygenic score derived from DNA alone, because the score reflects average risk in a population while the imaging reflects the specific structure of this specific dog. Polygenic tools can add useful information on top of phenotype evaluation, but they should not replace it.
Polygenic scores are also sensitive to the population they were developed in. A score built on one breed may perform poorly when applied to another, and a score built on one demographic generation may drift over time as allele frequencies and environmental contexts change. Good polygenic tools are validated specifically for the population being tested, and the validation work should be available for review. Families and breeders have a right to ask about validation before treating polygenic results as load-bearing in any decision.
4. Ancestry and diversity panels
These tests do not mainly predict disease. They describe the dog's place in population structure, including breed composition (useful for mixed-breed identification and for detecting unexpected ancestry), relatedness to other dogs in a reference database, genomic homozygosity and inbreeding estimates, and overall diversity metrics. Ambiguous Some panels also provide genomic COI estimates that are more accurate than short-window pedigree COI, especially in populations with incomplete pedigree records or hidden relatedness.
That information can be useful for breeding strategy and population management. A breeder who is actively managing diversity can use genomic COI estimates, runs of homozygosity analysis, and relatedness metrics to avoid matings that would concentrate the gene pool further, and those are legitimate uses of the tools. Programs that rely on diversity panels for their long-term planning are using the tests appropriately.
But ancestry and diversity panels do not, by themselves, tell you whether an individual dog will be healthy. They describe the dog's population position, not its clinical outcome. A dog with an excellent diversity profile can still develop disease, and a dog with a less ideal diversity profile can still live a long healthy life. Diversity information is population-level information that informs population-level decisions, not individual-level health predictions.
Why this four-part distinction matters
This four-part distinction is the central practical lesson of the page. Families often hear "DNA tested" and assume it means one thing, usually something like the causal-variant Mendelian testing that deserves the highest confidence. The field is really answering several different kinds of questions with very different levels of certainty, and the same panel report can contain results from all four categories mixed together without clearly indicating which is which.
A responsible breeder who uses DNA testing well can explain which tests on their panel fall into which category, why some results deserve more confidence than others, and how they combine testing with other screening layers to make breeding decisions. A breeder who treats all DNA test results as equivalent or who cannot explain the distinctions is either not understanding the tools they are using or is deliberately blurring the distinctions to sound more impressive than the underlying work supports.
Why It Matters for Your Dog
What This Cannot Predict
No genetic test guarantees lifelong health. Even the combination of the best causal-variant Mendelian tests, the most thoroughly validated marker tests, the best polygenic scores, and the best diversity panels cannot guarantee that any specific dog will not develop disease during its lifetime. Documented Genetic testing reduces risk at specific loci; it does not eliminate all health possibilities.
No clean disease-locus panel replaces orthopedic, cardiac, ocular, or behavioral evaluation. Phenotypic screening of the actual dog's actual body remains essential for traits that genetic testing can only estimate probabilistically.
No polygenic score turns probability into certainty. The score is a probability statement by design, and treating it as a verdict misunderstands what the tool is doing.
No diversity panel can be read as a direct health certificate for one dog. Diversity information is population-level context, not individual-level diagnosis.
And no genetic test today can cover the full catalog of conditions that may affect a breed. The catalog of known canine disease mutations continues to grow, and today's comprehensive panel will look incomplete in a decade as new causal variants are discovered.
That is why genetic testing should be treated as one layer in a wider screening architecture rather than as the architecture itself. The best breeders combine molecular testing with phenotypic evaluation, line knowledge, population management, and honest communication about what each tool does and does not do.
Families usually want a simpler answer than the science can give. They want to know whether the puppy they are about to bring home is healthy, and they are hoping that a DNA panel result can provide that answer in a few clean lines. Genetic testing helps with that question but only by answering specific narrower versions of it, not by delivering a global health verdict.
A better way to evaluate breeder testing is to ask more specific questions. What kind of test is this, and which of the four categories does it fall into? Is it a causal mutation test, a linked marker, a polygenic estimate, or a diversity panel? What exactly does the result rule in or rule out, and how confident should I be in the result for this specific breed? What other screening layers are you using alongside it, and how do those layers compensate for what DNA testing alone cannot see?
That last point matters because the strongest breeders do not rely on DNA testing alone. They combine molecular testing with phenotype-based screening in the domains where phenotype is the stronger tool (orthopedic imaging for joints, cardiac exams for heart conditions, ophthalmologic exams for eyes, behavioral observation for temperament) and with long-term line knowledge that captures patterns DNA testing cannot detect. A breeder who presents DNA testing as a comprehensive alternative to this integrated approach is overselling the tools.
For JB, this integrated approach is the only honest one. The program should use the high-confidence parts of canine genetics where they exist (validated Mendelian causal-variant tests for known Golden Retriever disease loci), treat the more conditional parts as conditional (linked markers, polygenic scores, diversity panels), and never speak about any test with more certainty than the test can actually carry. The goal is not to use the fewest tests or the most tests but to use each test at its appropriate confidence level and to combine them honestly with the other screening layers that genetic testing cannot replace. Families who understand the distinctions can evaluate the program's work on its merits. Families who have been given a simpler marketing version of the story will eventually discover the gap, and when they do, trust suffers. Honesty about what testing can and cannot do is ultimately the more sustainable communication strategy.
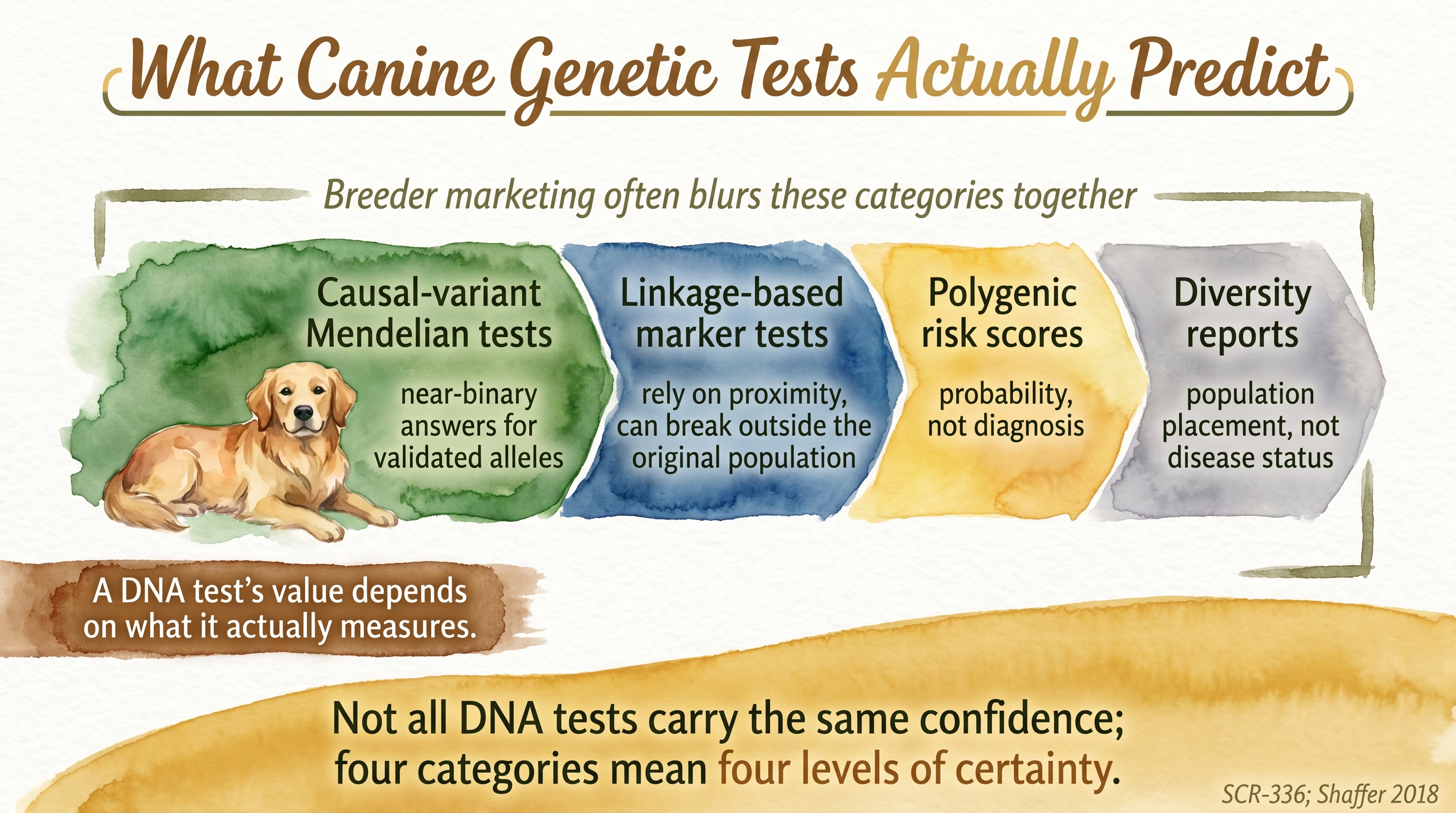
Not all DNA tests carry the same confidence; four categories mean four levels of certainty.
Key Takeaways
- Canine genetic tests do not all mean the same thing; some are causal mutation tests, others are marker tests, polygenic scores, or diversity reports.
- Causal-variant Mendelian tests are usually the strongest and most directly actionable form of canine DNA testing.
- Marker-based and polygenic tests are informative but inherently more conditional and probabilistic.
- Diversity panels describe population position rather than individual disease risk.
- The most honest breeder view is that genetic testing is one screening layer among several, not a guarantee of health.
The Evidence
This entry uses ambiguous claim-level tags beyond the dedicated EvidenceBlocks below. These tags mark claims where the literature remains unsettled or multiple interpretations coexist.
- Canine inherited-disease and testing literaturedogs
Canine DNA testing includes high-confidence mutation-specific Mendelian tests, linkage-based marker tests, polygenic risk models, and ancestry or diversity panels, each answering a different kind of question. - Canine validation frameworkdogs
The interpretive strength of a genetic test depends on whether it identifies a causal variant, a linked marker, or a probabilistic association profile.
- Canine complex-trait and diversity literaturedogs
Polygenic scores and diversity metrics can inform risk and population management, but they do not replace phenotype-based screening or guarantee individual outcomes. - Breed-specific validation literaturedogs
Marker-based and polygenic tests often fail to transfer cleanly across breeds because of differences in linkage disequilibrium structure and allele frequencies, making breed-specific validation an important prerequisite for reliable interpretation.
No comprehensive analysis has quantified the overall predictive accuracy of commercial canine DNA panels when all four test categories are combined into a single health assessment for one individual dog.
SCR References
Sources
- Shaffer L.G., Sundin K., Geretschlaeger A., Segert J., Swinburne J.E., Royal R., Loechel R., Ramirez C.J., & Ballif B.C. (2018). Standards and guidelines for canine clinical genetic testing laboratories. Human Genetics, 138(5), 493-499. doi:10.1007/s00439-018-1954-4
- Slutsky J., Officer A., & Giger U. (2013). A web resource on DNA tests for canine and feline hereditary diseases. The Veterinary Journal, 197(2), 182-187. doi:10.1016/j.tvjl.2013.02.021
- Farrell L.L., Schoenebeck J.J., Wiener P., Clements D.N., & Summers K.M. (2015). The challenges of pedigree dog health: approaches to combating inherited disease. Canine Genetics and Epidemiology, 2, 3. doi:10.1186/s40575-015-0014-9
- Awano T., Johnson G.S., Wade C.M., Katz M.L., Johnson G.C., Taylor J.F., Perloski M., Biagi T., Baranowska I., Long S., March P.A., Olby N.J., Shelton G.D., Khan S., O'Brien D.P., Lindblad-Toh K., & Coates J.R. (2009). Genome-wide association analysis reveals a SOD1 mutation in canine degenerative myelopathy that resembles amyotrophic lateral sclerosis. Proceedings of the National Academy of Sciences, 106(8), 2794-2799. doi:10.1073/pnas.0812297106
- Zeng R., Coates J.R., Johnson G.C., Hansen L., Awano T., Kolicheski A., et al. (2014). Breed distribution of SOD1 alleles previously associated with canine degenerative myelopathy. Journal of Veterinary Internal Medicine, 28(2), 515-521. doi:10.1111/jvim.12317
- Ivansson E.L., Megquier K., Kozyrev S.V., Murén E., Körberg I.B., Swofford R., et al. (2016). Variants within the SP110 nuclear body protein modify risk of canine degenerative myelopathy. Proceedings of the National Academy of Sciences, 113(22), E3091-E3100. doi:10.1073/pnas.1600084113
- Ginja M., Gaspar A.R., & Ginja C. (2015). Emerging insights into the genetic basis of canine hip dysplasia. Veterinary Medicine: Research and Reports, 6, 193-202. doi:10.2147/VMRR.S63536
- Tonomura N., Elvers I., Thomas R., Megquier K., Turner-Maier J., Howald C., et al. (2015). Genome-wide Association Study Identifies Shared Risk Loci Common to Two Malignancies in Golden Retrievers. PLOS Genetics, 11(2), e1004922. doi:10.1371/journal.pgen.1004922